Engaging patient & public partners in a scoping review on the science and practice of James Lind Alliance Priority Setting Partnerships
Alexandra Korall, Maya Jeyaraman, Tamara Rader, Carolyn Shimmin, Sharon Straus, Christina Weise and Kathryn Sibley
Café Scientifique “The Fallout – Research & Practical Tips for Preventing Falls”
Implementation of Balance and Fall Prevention Evidence: Unlocking the Key Ingredients
 Fall Prevention: Targeted Exercise Reduces Risk
Fall Prevention: Targeted Exercise Reduces Risk
By Jennifer Van Pelt, MA
Today’s Geriatric Medicine
Vol. 14 No. 4 P. 28
With age, the risk of falling increases and the ability to bounce back after a fall decreases. According to the Centers for Disease Control and Prevention (CDC), 36 million older adults fall each year—and more than 32,000 die from fall-related complications. Every year, 3 million older adults visit emergency departments for injuries from a fall. One in five falls causes a serious injury, such as a broken bone or head trauma, and more than 95% of hip fractures in older adults result from a fall. And, after falling once, the chance of falling again is doubled.1 Many older adults may never fully recover from a fall, suffering reduced mobility, decreased quality of life, and further health decline.
Numerous other factors besides age and previous falls contribute to the risk of falling in older adults. The CDC notes that most falls are caused by the interaction of multiple risk factors—the more risk factors, the greater the risk of falling. These other risk factors can include the following:
• use of certain medications;
• muscle weakness;
• gait and balance problems;
• vision impairment;
• postural hypotension; and
• medical conditions and diseases such as arthritis, stroke, diabetes, dementia and Parkinson’s disease, multiple sclerosis, vestibular disorders, and postural hypotension.
A February 2021 study found that older adults with markers of frailty (eg, fatigue, weakness, weight loss, low physical activity, poor balance, and cognitive impairment) are as much as 53% more likely to experience multiple falls.2
Several of these risk factors for falling can be addressed with regular exercise; improving strength, balance, and flexibility can help reduce the likelihood of falling and fall-related injuries. Targeting exercise specifically for fall prevention can reduce fall risk even more.
Research has shown that exercise is the most effective intervention for fall prevention in older adults. In general, more active older adults have a lower risk of falling than do those who are less active, and popular exercise activities for older adults, such as low-impact aerobics, tai chi, strength training, and yoga, can provide benefits related to balance, coordination, and flexibility that help to prevent falls.
Recent research has also highlighted the most effective exercises for fall prevention. A November 2020 pooled analysis of 116 randomized controlled trials that included 25,160 participants aged 60 years or older found that exercise reduced the rate of falls by 23%. Subgroup analyses found that different types of exercise were associated with the same or greater reductions in fall risk. Tai chi reduced fall risk by 23%. Balance and functional exercises were associated with a 24% reduction. A combination of balance and functional exercises with resistance training was found to reduce fall risk by 28%. Performing three or more hours weekly of balance and functional exercises was found to reduce falls by 42%.3
Another November 2020 analysis also evaluated the comparative effectiveness of fall prevention exercise interventions.4 “We analyzed data from 73 studies including more than 30,000 participants to identify effective components of fall prevention exercise. We found that the most effective exercise for reducing the number of older adults who fall included four types of balance—anticipatory, reactive, dynamic, and functional—as well as flexibility,” explains Kathryn Sibley, PhD, Canada Research Chair in Integrated Knowledge Translation in Rehabilitation Sciences, an associate professor at the University of Manitoba, and lead author of the meta-analysis.
Sibley and her colleagues reviewed and analyzed randomized controlled trials comparing different exercise types or comparing exercise with no exercise or usual care to evaluate number of older adults who fell and fall injuries. The mean age of study participants ranged between approximately 65 and 92 years.4
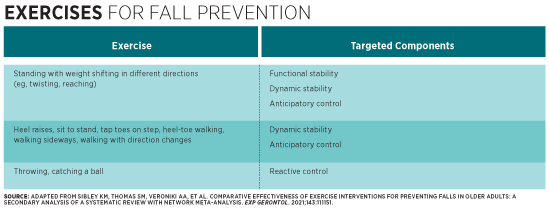
Five exercise components were found to be most effective for reducing the number of older adults who fall, including flexibility and the following four components of balance—balance being defined as the ability to maintain control of one’s center of mass in relation to a base of support4:
• functional stability, defined as the ability to move one’s center of mass as far as possible in any direction within the base of support (eg, being able to reach for something without losing balance);
• dynamic stability, defined as the ability to maintain one’s center of mass position when the base of support changes (eg, moving from seated to standing, or when walking);
• anticipatory control, defined as the ability to move one’s center of mass position in advance of a voluntary movement that would otherwise cause instability (eg, walking up steps); and
• reactive control, defined as the ability to recover stability after one’s center of mass moves beyond the base of support (eg, stopping oneself from falling after tripping).
“This analysis is very exciting because for the first time we have unlocked the key ingredients for fall prevention exercise. We can use this information to design more precise exercise programs that target these critical components and more effectively help older adults stay mobile and active by preventing more falls,” Sibley notes.
Those working with geriatric patients can incorporate these components of balance and flexibility into exercise programs for older adults, Sibley emphasizes. In their analysis, Sibley and her colleagues listed some sample exercises that target each balance component (see table).
In combination with flexibility exercises, such as stretching and gentle yoga, exercises homing in on the four balance components identified by Sibley and her colleagues may improve the effectiveness of existing fall prevention programs. Many of these programs already include such components, as do fitness classes geared toward older adults, such as Silver Sneakers, and tai chi.
These balance exercises can also be combined with resistance training to improve muscular strength and bone density, as well as provide a challenge for more active older adults. For example, adding a handheld weight or a resistance band to a standing twist and reach exercise adds core and upper body strengthening to a balance exercise that targets functional and dynamic stability and anticipatory control. Holding weights while rising from seated position to standing or doing heel raises adds lower body muscular strength and endurance to a balance exercise that targets dynamic stability and anticipatory control. Tossing weighted bean bags or bouncing and catching a lightweight medicine ball adds upper body strengthening to a reactive control exercise.5
Unfortunately, those older adults who most need to exercise for fall prevention tend not to. It may be more challenging to motivate less active and frailer older adults to exercise. In a group fitness setting, less active and frailer older adults may view more active and fit participants as intimidating. Or, even though most exercises can be adapted to a lower level of fitness or to chair exercises, frail older adults may feel self-conscious or embarrassed to need modifications, which may prevent them from accessing appropriate programs. And, ironically, a fear of falling is a common barrier to exercising for fall prevention, especially in older adults who have fallen previously, have a medical condition or disability, or experience depression.6
Research suggests that initiatives to increase fall prevention awareness in the community setting and stressing its importance to those who care for geriatric populations (eg, assisted living facility staff, primary care providers) can help improve older adult participation in fall prevention exercise programs. For example, church-based and community recreation center fall prevention information and classes, as well as programs delivered in the primary care setting, have been shown not only to improve access to and participation in fall prevention but also to reduce fear of falling.6-8
Given that targeted exercise programs are the most effective intervention to prevent falls, expanding awareness and access to them is essential to reduce the high number of older adults who fall each year and the consequences of those falls.
A Delicate Balance

“Balance is not just one sense, but a complex puzzle comprised of many interlocking pieces, including stability, strength, range of motion, the ability to anticipate and react.”
A research collaboration between Deer Lodge Centre and the University of Manitoba aims to give therapists better tools for assessing falls risk.
By Ryan McBride
Not falling over is harder than you think. Or at least it’s more complicated: the interactions of brain, muscle and sensation that go into keeping us upright under even the best of circumstances are subtle and varied. The ability to maintain balance is like a delicate gyroscope wired into our senses, our muscles, and our ability to react to anything that might throw us off: the edge of a carpet, a patch of uneven ground, or ill-fitting footwear.
Under less ideal circumstances, or when there are impairments in the body’s systems that maintain balance, staying upright proves to be a challenge many people know all too well.
One of the most dangerous consequences of compromised balance is a bad fall, which can lead to serious and sometimes life-threatening injuries. Bad falls are also an all-too-common reason for admission among the many clients requiring care from Deer Lodge Centre’s geriatric rehabilitation program—so when a researcher from the University of Manitoba approached the Centre about exploring a new test that might help physiotherapists better assess their clients’ risk of falling, the answer was a hard yes.
“A complex puzzle”
Kathryn Sibley is an assistant professor in the U of M’s department of Community Health Sciences and a scientist in the Knowledge Translation Platform at the Centre for Healthcare Innovation. She’s interested in why people fall, and in testing tools clinicians can use to assess and treat fall patients.
“Balance is not just one sense, but a complex puzzle comprised of many interlocking pieces, including stability, strength, range of motion, the ability to anticipate and react,” she says. “Even simply identifying the pieces themselves is the subject of a great deal of research going on right now. We keep discovering new pieces. Then we have to figure out how they interlock with the other pieces we know keep us standing upright.”
Several years ago, another group of balance researchers developed a comprehensive test to measure the performance of each puzzle piece in people of all ages and backgrounds. A more concise and user-friendly version of the test, designed for clinicians to use on the job, came soon after. It’s this version—the Mini BESTest—that Deer Lodge clients and clinicians will work with Sibley to assess.
In January, Sibley and her team will begin training physiotherapists at Deer Lodge Centre to conduct the project, which is funded in part by a substantial grant from the Deer Lodge Centre Foundation. Over the next eight months, they will perform the Mini BESTest on approximately 65 patients and residents on the Centre’s geriatric rehabilitation units—older adults who are recovering from illness, injury or age-related frailty, and who display evidence of balance impairment. Participants will be assessed on their ability to complete 14 activities, including stepping over obstacles, standing on one leg, and turning while walking.
“A tool that works”
Cara Windle, Deer Lodge’s Clinical Service Leader for Physiotherapy, says she and her colleagues are excited about the project because there’s a definite need in their profession for more meaningful and thorough balance assessment tools.
“Many of our clients are functioning at a very low level,” she explains. “It’s very challenging to find a tool that works for those folks, rather than something aimed specifically at people who are well enough, for instance, to still live on their own in the community.”
While Sibley believes the Mini BESTest, or aspects of it, may provide the right solution, the test hasn’t been studied on geriatric rehabilitation patients.
Each participant will be tested twice. “Obviously the first thing we want to know is how valid and reliable the test is for geriatric rehab patients. Can they even use this test? How many of the activities it measures are they able to perform?”
Testing twice will help researchers establish what scores constitute a meaningful improvement.
Sibley and her partners will also compare the scores to those from other tests commonly employed. Establishing this basis for comparison is key, Sibley says, because it places the project’s results into a useful context for other researchers around the world.
Ultimately, she says, “The data we collect will help Deer Lodge and other facilities like it serve their patients better, and make more informed decisions about how they might adopt the test.”
“Close to the edge”
Physiotherapists treating balance problems face a common conundrum: How do you challenge a patient’s balance to accurately assess the limits of their abilities, while managing their safety?
Susan Bowman, Manager of Physiotherapy at Deer Lodge, and one of the project’s facilitators, says that in some cases, “therapists struggle to find ways to challenge patients and take them close to the edge of maintaining their balance because of the risks of causing a fall. On the other hand, we need to get closer to that edge for a more accurate assessment.”
Sibley says the Mini BESTest may offer a solution through how it assesses reactive balance, a skill that helps us recover when our balance is challenged. “When you or I trip on a rug, we have this rapid muscle response that helps us recover. It feels automatic. But someone older or with compromised balance may not have that same response. This test has a very specific procedure to challenge the limits of a client’s balance by triggering that reaction while using strategies to keep them safe and secure.”

This is important to clinicians such as Windle. She’s concerned that test results, usually conducted in a controlled in-patient setting, don’t always indicate how patients will cope with the less predictable environment they encounter at home. “That lack of reactive balance is often what leads to falls that bring people here, or brings them back here,” she says.
Windle, Sibley and their collaborators hope that the Mini BESTest will demonstrate enough sensitivity to measure the abilities of clients with vastly different functional abilities, from the relatively mobile to the profoundly frail. “Just because someone does very well on one test doesn’t mean they aren’t still at risk for a fall,” says Bowman. “It just means the test may not be sensitive enough to challenge them where their balance is weak.”
Windle offers an example. “Sometimes we ask a patient to do a Timed Up and Go test, where they stand from a chair, walk a certain distance, and come back to the chair. That gives us a sense of their risk for falling, and it’s very simple. But although there’s good evidence that suggests the score correlates with their risk of falls, we know the test is too simple to give us all of the information we require to make an informed recommendation about risk.”
“The best service out there”
Another benefit of the Mini BESTest is its scoring system, which provides an overall score along with scores for individual components of balance—vital information that can help clinicians zero in on specific components affecting poor balance, or identify factors beyond the scope of the test, such as impaired vision, dizziness due to low blood pressure, or other medical, environmental or cognitive issues, that may be contributing to the problem. Knowing the specific causes of an individual’s balance problem will help therapists devise more appropriate exercise programs and recommendations for additional therapeutic or coping strategies.
But patients aren’t the study’s only participants. Researchers are also keen to find out how the Mini BESTest helps the physiotherapists using it. Physiotherapists will themselves become research participants: once the trial is complete, they’ll be asked how easy the test was to complete, and how it changed their actual practice. “Even if it’s effective, if it’s too complicated to use in a hectic, fast-paced rehab ward, no one’s going to use it,” Sibley says.
Susan Bowman believes the test may offer clinicians the means of achieving an even better balance of care in their own practice: “We hope the results will tell us how we can challenge our staff, to help them continue to learn and grow and offer the best service out there.”
originally published on www.deerlodgefoundation.ca
